Introduction to Nursing Assessment

Nursing assessment is a crucial step in the nursing process that involves gathering information about a patient’s physical, emotional, and psychological health. This information is used to identify the patient’s needs, develop a care plan, and evaluate the effectiveness of interventions. A thorough nursing assessment is essential to provide high-quality patient care. In this article, we will discuss five nursing assessment tips that can help nurses to conduct a comprehensive assessment.
Tip 1: Start with a Comprehensive Health History

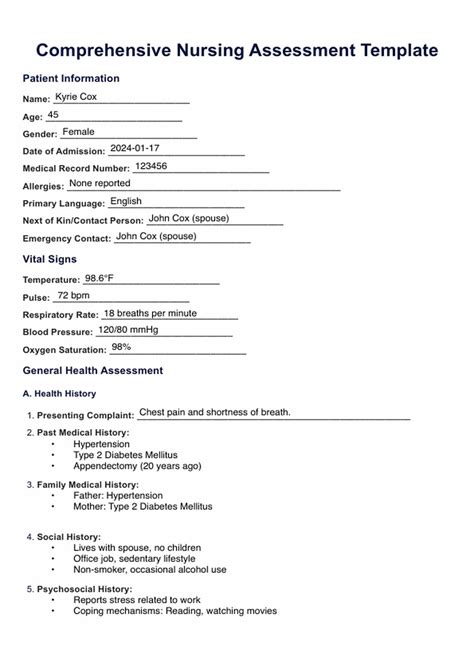
A comprehensive health history is the foundation of a nursing assessment. It involves gathering information about the patient’s medical history, including previous illnesses, surgeries, and hospitalizations. Nurses should also ask about the patient’s family medical history, allergies, and medications. This information can help identify potential health risks and inform the development of a care plan. Some key questions to ask when taking a health history include: * What is your chief complaint? * What is your medical history? * What medications are you currently taking? * Do you have any allergies? * What is your family medical history?
Tip 2: Conduct a Thorough Physical Assessment

A physical assessment involves evaluating the patient’s physical health, including their vital signs, body systems, and overall physical condition. Nurses should use their senses to observe, listen, and feel the patient’s body to gather information. Some key components of a physical assessment include: * Vital signs: temperature, pulse, blood pressure, respiratory rate, and oxygen saturation * Body systems: cardiovascular, respiratory, neurological, gastrointestinal, and genitourinary * Physical condition: skin, hair, nails, and overall appearance
Tip 3: Use Standardized Assessment Tools

Standardized assessment tools can help nurses to conduct a comprehensive and systematic assessment. These tools can include questionnaires, scales, and checklists that are designed to evaluate specific aspects of a patient’s health. Some examples of standardized assessment tools include: * The Braden Scale for predicting pressure sore risk * The Morse Fall Scale for assessing fall risk * The Confusion Assessment Method (CAM) for evaluating delirium
Tip 4: Consider the Patient’s Cultural and Spiritual Needs

A patient’s cultural and spiritual needs can have a significant impact on their health and well-being. Nurses should consider these needs when conducting a nursing assessment and developing a care plan. Some key questions to ask when assessing cultural and spiritual needs include: * What is your cultural background? * What are your spiritual beliefs and practices? * How do you prefer to communicate? * What are your dietary preferences and restrictions?
Tip 5: Document Your Findings Accurately and Completely
Accurate and complete documentation is essential for nursing assessment. Nurses should document their findings in a clear and concise manner, using standardized terminology and formatting. This documentation can help to inform the development of a care plan and evaluate the effectiveness of interventions. Some key principles of documentation include: * Be accurate and complete * Use standardized terminology and formatting * Document findings in a timely manner * Use electronic health records (EHRs) when available
📝 Note: Documentation is a critical component of nursing assessment, and nurses should prioritize accuracy and completeness when recording patient information.
As we summarize the key points discussed in this article, it is clear that nursing assessment is a complex and multifaceted process that requires careful consideration of a patient’s physical, emotional, and psychological health. By following these five nursing assessment tips, nurses can conduct a comprehensive and systematic assessment that informs the development of a care plan and evaluates the effectiveness of interventions. The tips provided can help nurses to identify potential health risks, develop a care plan, and evaluate the effectiveness of interventions, ultimately leading to better patient outcomes.
What is the purpose of a nursing assessment?
+
The purpose of a nursing assessment is to gather information about a patient’s physical, emotional, and psychological health, which is used to identify the patient’s needs, develop a care plan, and evaluate the effectiveness of interventions.
What are the key components of a physical assessment?

+
The key components of a physical assessment include vital signs, body systems, and overall physical condition, such as skin, hair, nails, and appearance.
Why is documentation important in nursing assessment?

+
Documentation is important in nursing assessment because it provides a permanent record of the patient’s health status, informs the development of a care plan, and evaluates the effectiveness of interventions.